I secured a small grant to investigate UK residents’ perceptions of contact tracing apps. I am just waiting for ethical approval, before I can start collecting data via interviews and, after that, a survey. In the meantime, I am checking the latest published research on related topics.
Based on my previous work, I know that there are three types of factors that impact on the adoption and sustained use of health enhancing apps and devices. There are factors about:
- The technology itself – e.g., features
- The context of use. This includes the technical context (e.g., network coverage), and the social context (e.g., whether others can see the user use the app).
- The user, including their characteristics and attitudes.
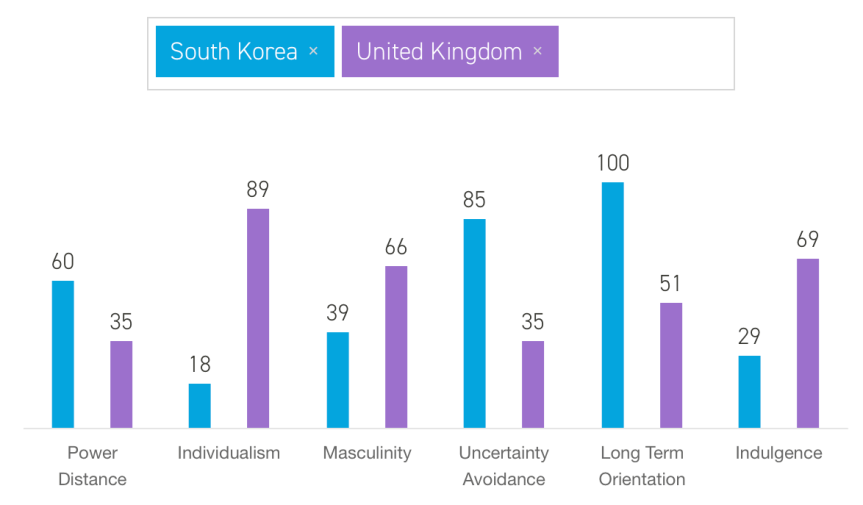
In terms of the user, narratives about the “success” of contact tracing apps in countries like South Korea, note that citizens of those countries are collectivist and that they place a lot of trust in their governments to do the right thing. Both arguments spell disaster for the app’s adoption in the UK:
However, broad cultural characteristics are too crude an approach to understand individual users’ behaviours. Clearly, UK citizens don’t always act in ways that are consistent with an ego-centric, self-reliant ethos; just like not all South Korean citizens consistently display blind-trust in their politicians. So, a more refined understanding of the values and motivations underpinning proactive health-management behaviours is needed, for this research project.
A recently published paper offered me an interesting avenue for exploration. This paper was authored by Janet Davey, Judith Herbst, Raechel Johns, Joy Parkinson, Rebekah Russell-Bennett and Nadia Zainuddin, and was published in Journal of Service Theory and Practice. A free version is available here. The paper is entitled “The role of health locus of control in value co-creation for standardized screening services”, and examines participation in standardised, voluntary disease screening services. The context is cancer screening services. Obviously, COVID-19 and cancer are very different diseases; and contact tracing apps are very different from cancer screening exams. Still, there is one finding from the research reported in the paper that may be very relevant for this research project: health locus of control (HLOC).
What is (health) locus of control?
Locus of control is a personality attribute, and refers to where someone places the responsibility for the outcome of events in their lives. For instance, when you order the wrong item online, do you blame yourself (e.g., I wasn’t paying attention) or do you blame others (e.g., the website was poorly designed)?
If you attribute the responsibility of the outcome to yourself, you are said to have an internal locus of control. Conversely, if you attribute the responsibility of the outcome to others, you are said to have an external locus of control.
An internal health locus of control means that people tend to believe that their health outcomes depend on their own actions, such as what they eat, or how much they exercise. In turn, an external health locus of control means that people attribute their health outcomes to factors such as genetics or luck.
What is the relevance of health locus of control for disease screening programmes?
Locus of control doesn’t tell us whether someone will be more or less inclined to manage their health – namely, whether someone will be more or less inclined to participate in disease screening programmes. However, locus of control can tell us which approaches are more likely to resonate with different individuals.
When it comes to participation in disease screening programmes, Davey and her colleagues found that HLOC mattered in terms of benefits obtained, and the level of effort invested.
A) Benefits
By and large, people participated in cancer screening programmes as a means of staying free from the disease. However, for people with internal locus of control, participating in the screening provided them with personal satisfaction, and even a feeling of happiness, that they were doing something to enhance their health. In contrast, for those with external locus of control, the main driver was to reduce the stress caused by factors beyond their control, and they were mostly concerned with addressing worry.
Moreover, those with internal HLOC had a focus on the long-term horizon: they believed that participating in screening activities would help advance science (e.g., adding to national databases), such that, ultimately, they as well as others would stay well and healthy for longer. These persons derived what Davey and her colleagues called the “we-value”. Instead of increasing positive emotions in the long term, those with external HLOC focused on avoiding or reducing short term negative emotions.
B) Effort
Those with internal HLOC were willing to exert additional effort to stay safe. For instance, taking the initiative of scheduling appointments, or engaging in self-checking in between appointments.
In contrast, those with external HLOC focused on minimising efforts. That is, they relied on others telling them what to do, not just medical professionals, but also family and friends. They appreciated things like reminders, and they would just do enough to keep their – or their loved ones’ – worries at bay.
Impact on disease screening programme’ mechanisms
Due to the different type of benefits sought, and the different level and type of effort that people are prepare to put into disease screening, health providers need a variety of mechanisms to engage with users of their services.
The authors of the “The role of health locus of control in value co-creation for standardized screening services” paper suggest the following activities to target users with external vs internal HLOC:

Having read this paper, I am now thinking about how the HLOC framing might help me understand whether UK residents will download and use contact tracing apps. What are your thoughts? Also, if you would like to participate in this study, do let me know. Interviews will start soon, and will be conducted via video conferencing.

